
Problems with Electronic Health records
An electronic health record (EHR) is a digital version of a patient’s paper chart. EHRs are real-time, patient-centered records that make information available quickly and securely to authorized users.
EHRs are designed to be shared with other providers and to aid the level of care provided across the care continuum. It also allows you to track additional patient information. It contains the medical and treatment histories of patients, an EHR system is built to go beyond standard clinical data collected in a provider’s office and can be inclusive of a broader view of a patient’s care. EHRs are an important part of health IT and can:
- Contain a patient’s medical history, diagnoses, medications, treatment plans, immunization dates, allergies, radiology images, and laboratory and test results
- Allow access to evidence-based tools that providers can use to make decisions about a patient’s care
- Automate and streamline provider workflow
One of the key features of an EHR is that health information can be managed and created by authorized providers in a digital format capable of being shared with other providers across more than one health care organization. EHRs are built to share information with other health care providers and organizations – such as laboratories, specialists, medical imaging facilities, pharmacies, emergency facilities, and school and workplace clinics – so they contain information from all clinicians involved in a patient’s care.
With EHRs, your organization can help build a healthier future for our nation.
- Potential Privacy and Security Issues: As with just about every computer network these days, EHR systems are vulnerable to hacking, which means sensitive patient data could fall into the wrong hands.
Inaccurate Information: Because of the instantaneous nature of electronic health records, they must be updated immediately after each patient visit — or whenever there is a change to the information. The failure to do so could mean other healthcare providers will rely on inaccurate.
How to Fix Problems with Electronic Health Records:

Optimize costs and improve the efficiency of the system.
Implement seamless documentation flow
A clinic processes a ton of documentation. Most of it records information about the patient and the provided care (known as evaluation and management (E/M) documentation), which is important not only to monitor the patient’s health but also to ensure accurate payment for services and insurance coverage.
Another type of documentation – documentation for medication approval – is exchanged between healthcare providers, so they need to be compliant with industry-recognized standards.
Clinicians not only have to fill this documentation, but also comply with different sets of guidelines, and that cuts into their patient and personal time. Here’s how EHRs can help with that.
Today, most EHR providers make detailed document templates so that all the information needed for audit is recorded. But this means that healthcare workers are required to record all this information.
To experience the benefits of these and many other revisions, you need to actually adopt them within the EHR. This process includes:
- Making patient history information available from other systems using secure APIs
- Updating EHR design to support data verification instead of recording
- Creating new electronic workflows for a patient’s portal
While health IT solutions streamline the administrative processes, they also create a large discrepancy, each one developing different interfaces that clinicians need to learn and get used to. So, we need to make different systems work together seamlessly and also help end-users operate them with ease. Here are some options.
- Consulting with end-users when making decisions about displayed elements, alerts, the level of personalization, and so on
- Studying clinicians’ routines and work patterns and conducting interviews with them
- Optimizing third-party applications that clinicians already use
The main goal here is to make sure the software balances between industry regulations, day-to-day operations, and objective parameters like ease of use.
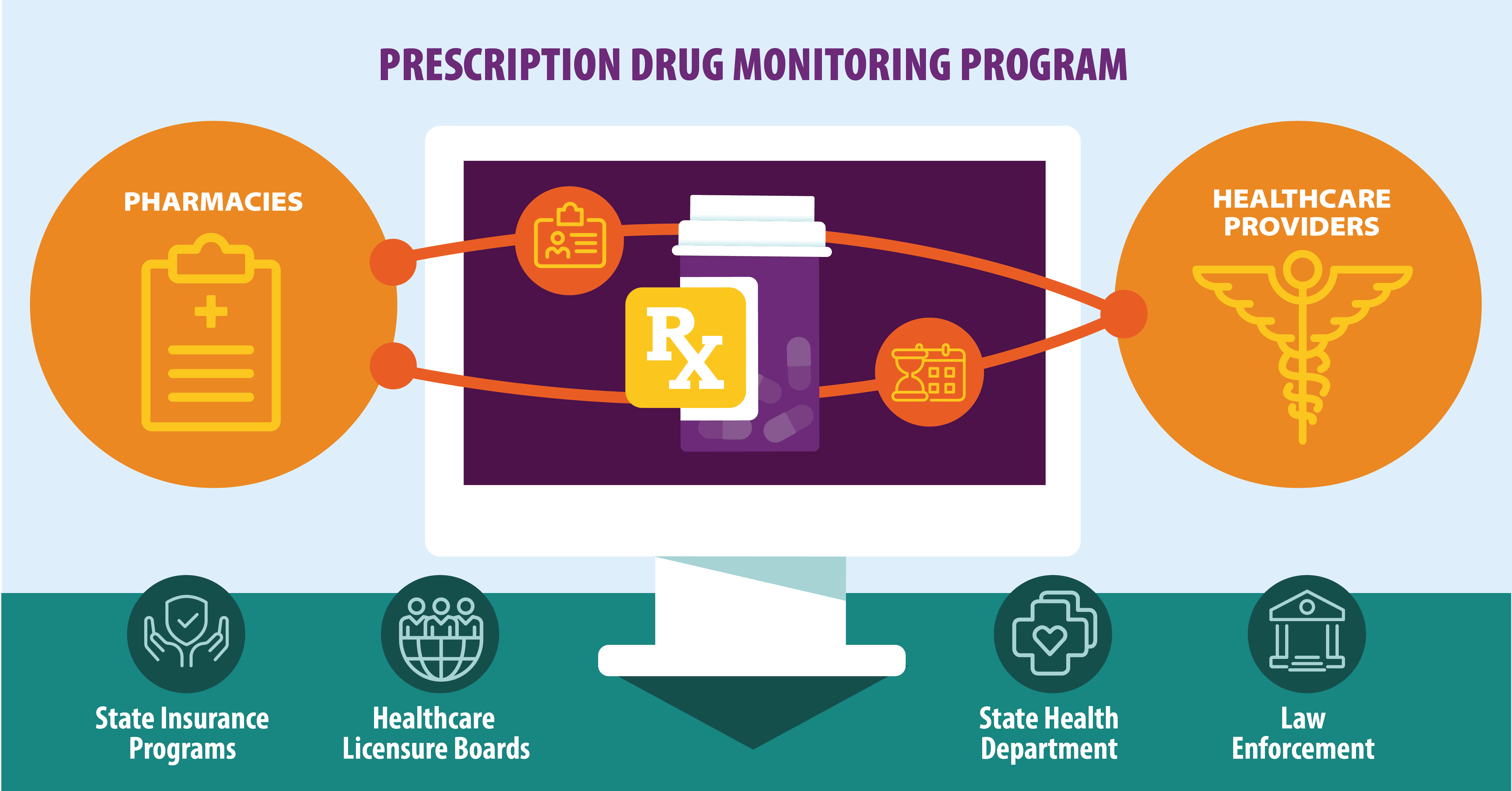
Set up automatic PDMP data access – an EHR should be able to access medication history automatically when a doctor writes a prescription or a patient is being admitted to the ER.
Set up automatic processing of PDMP requests – a patient’s demographic information is automatically passed from EHR to PDMP.
Establish formatted reports for PDMP data – PDMP data is always displayed in a formatted, user-friendly, and unified manner.
Set up automatic PDMP data storing – medication history is automatically recorded in a patient’s log.
The main challenge for implementing PDMP sharing in the EHR workflow today is a regulatory one. Medication history is, of course, extremely sensitive information and should be protected. So, EHRs and hospitals themselves must ensure that the information they obtain and store is well protected – meaning, they must be subject to HIPAA.
- Computer terminals should be physically guarded
- Each change in the system should be tracked and logged
Additionally, if EHR software has built-in security features, it should be configured properly, which is rarely done in an organization without a security team or specialist. So, the ultimate goal is assigning people responsible for the security and teaching the staff the main security rules.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment